

Quick Summary
| What You Want to Know | Answer |
|---|---|
| What is a hairline fracture? | A tiny, incomplete crack in a bone caused by repetitive stress or sudden force |
| Most common locations | Foot, shin (tibia), ankle, lower back |
| Key symptom | Dull, worsening pain that eases with rest |
| Does it show on X-ray? | Often not — MRI is the gold standard |
| Healing time | 6–8 weeks with proper rest |
| Can you walk on it? | Possible but not advisable — worsens the fracture |
| When is surgery needed? | Rarely — only for high-risk sites or complete displacement |
What Is a Hairline Fracture?
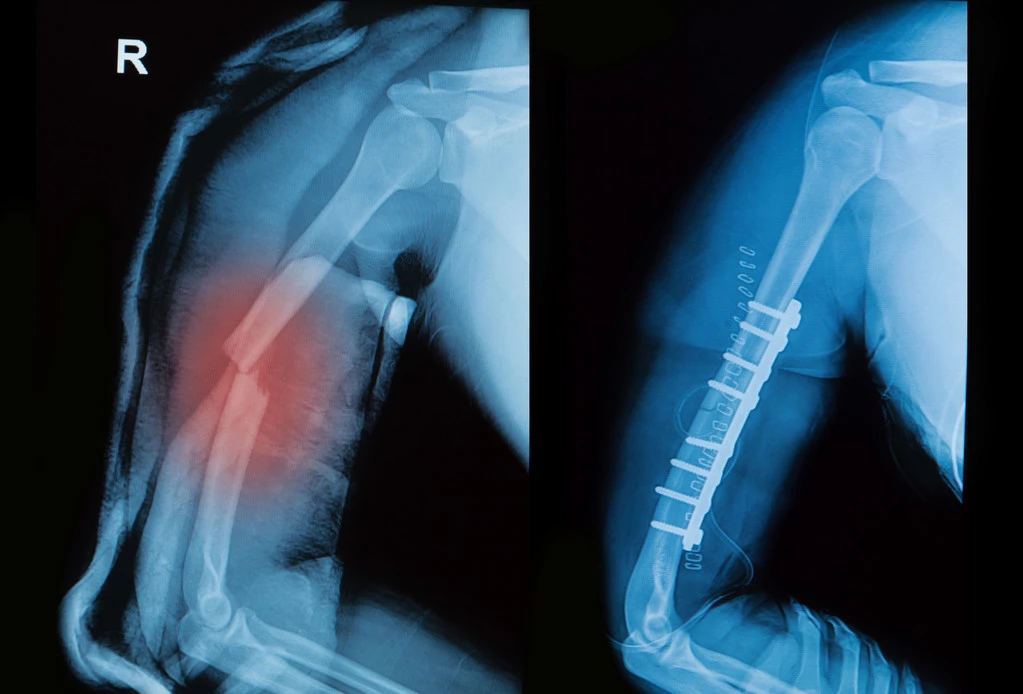
In over 20 years of treating patients in orthopedic clinics, hairline fractures are among the most underdiagnosed and most mistreated injuries I encounter. Patients walk in having “pushed through the pain” for weeks, sometimes turning a minor crack into a complete fracture that now needs surgery. The injury deserved far more respect than they gave it.
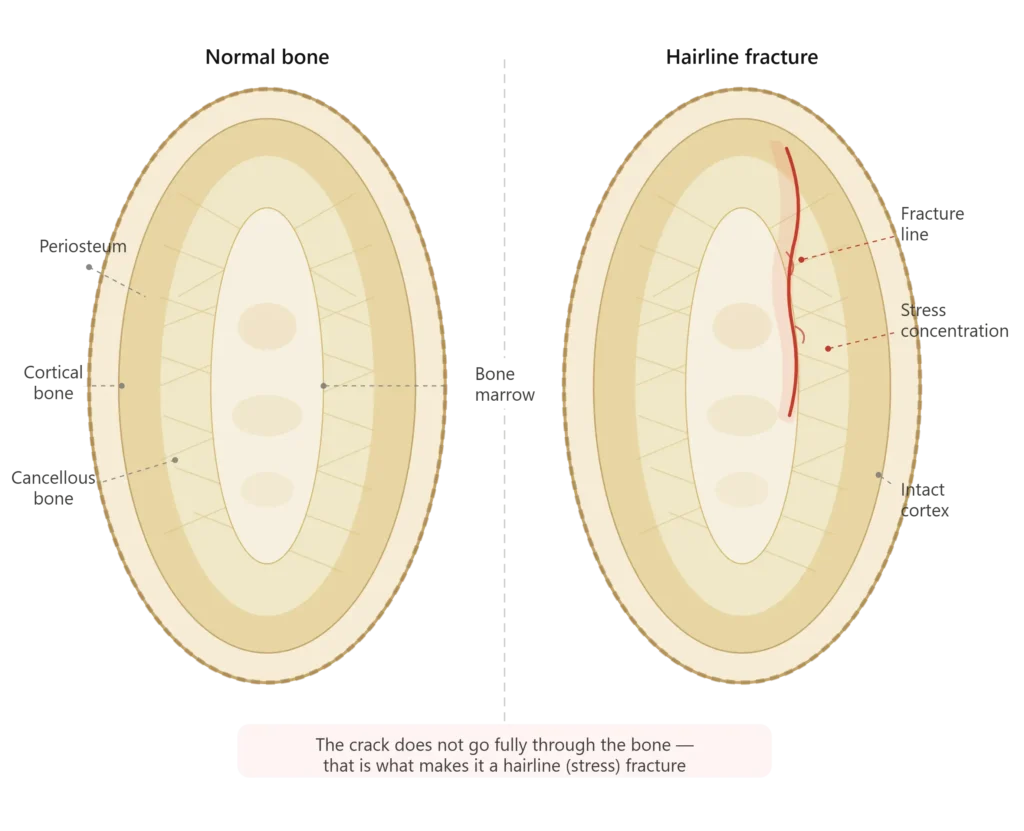
A hairline fracture — also called a stress fracture — is a small, incomplete crack within a bone. It does not go all the way through the bone (that would be a complete fracture), but it is a structural compromise that the bone cannot sustain under repeated loading.
Think of it this way: bend a metal paperclip back and forth repeatedly. Before it snaps completely, tiny cracks form in the metal. That is exactly what happens in the bone. The bone is strong enough to handle a single load, but when the same force is applied repeatedly without adequate recovery time, the microscopic damage accumulates faster than the bone can repair itself.
There are two main types:
- Stress fractures — result from repetitive, cumulative loading over time (common in athletes and soldiers)
- Insufficiency fractures — occur in bones already weakened by conditions like osteoporosis, even with normal activity levels
Both present similarly and are treated comparably, but the underlying cause shapes the long-term management plan significantly.
Where Do Hairline Fractures Most Commonly Occur?
The lower extremities absorb the majority of our body weight and impact forces, which is why most hairline fractures cluster in the legs and feet.
| Location | Common In | Notes |
|---|---|---|
| 2nd and 3rd metatarsals (foot) | Runners, soldiers, dancers | Most common site overall; called “march fracture” in military literature |
| Tibia (shin bone) | Runners, basketball players | Can progress to complete fracture without rest |
| Fibula (outer lower leg) | Runners, gymnasts | Often overlooked as an ankle sprain |
| Navicular (midfoot) | Sprinters, jumpers | High-risk site — poor blood supply, slow to heal |
| Calcaneus (heel bone) | Long-distance runners | Dull heel pain, often misdiagnosed as plantar fasciitis |
| Lumbar vertebrae (lower back) | Young athletes, especially gymnasts | Called spondylolysis — different presentation |
| Femoral neck (hip) | Older adults, distance runners | Serious — can lead to avascular necrosis if missed |
Surgeon’s note: Femoral neck and navicular fractures deserve special attention. These are what we call “high-risk” stress fracture sites due to poor blood supply and high mechanical loading. Miss these and you’re looking at non-union, avascular necrosis, or surgery. If you suspect a hip fracture in any form, do not delay seeking care.
Signs and Symptoms of a Hairline Fracture
The symptoms of a hairline fracture are deceptively mild early on — which is precisely what makes them dangerous. Patients continue activity, worsening the crack with every step.
The Classic Symptom Pattern
- Pain that builds gradually — not a sudden snap like a complete fracture; it starts as mild discomfort and intensifies over days to weeks
- Pain worsens with activity, relieves with rest — this is the most clinically reliable pattern I use to differentiate stress fractures from soft tissue injuries
- Point tenderness — pressing directly on the fracture site produces a sharp, localized pain; this is called the “hop test” or “fulcrum test” in clinical examination
- Mild swelling — present in most cases, especially around the foot and ankle
- Bruising — can occur in some cases but is less common than with complete fractures
How Hairline Fracture Pain Differs From a Sprain or Muscle Strain
| Feature | Hairline Fracture | Sprain / Muscle Strain |
|---|---|---|
| Onset | Gradual over days/weeks | Usually sudden |
| Location of pain | Precise, pinpoint | Diffuse, broader area |
| Tenderness | Directly on bone | Around ligament or muscle belly |
| Response to rest | Significantly improves | Slower, variable improvement |
| Night pain | Can occur | Uncommon |
| X-ray findings | Often normal initially | Always normal |
When to go to the emergency room: If you cannot bear any weight at all, if there is significant deformity, if the pain came on from a high-energy injury (car accident, hard fall), or if there is numbness — seek emergency care. These may suggest a complete fracture.
What Causes a Hairline Fracture?
The Bone Remodeling Imbalance
Healthy bone is not static. It constantly remodels — old bone is resorbed by cells called osteoclasts, and new bone is laid down by osteoblasts. Under normal activity, this process keeps your skeleton strong and responsive.
The problem arises when you increase the intensity, duration, or frequency of loading faster than the bone can adapt. The osteoclasts get to work breaking down fatigued bone, but the osteoblasts haven’t caught up yet. That window of imbalance is when a hairline fracture occurs.
Common Causes
- Training errors — the single most common cause; increasing running mileage too quickly, starting a new high-impact sport, adding too many training sessions per week
- Sudden change in surface — moving from grass to concrete, hard court to clay; each surface transmits forces to bone differently
- Improper or worn-out footwear — shoes without adequate cushioning fail to attenuate impact forces before they reach the bone
- Osteoporosis or low bone density — reduces the threshold at which bone can crack; even walking can cause stress fractures in severely osteoporotic individuals
- Nutritional deficiencies — low calcium, low Vitamin D, or the combination of low energy availability with intense training (seen frequently in female athletes — discussed below)
- Previous stress fractures — having one increases your lifetime risk significantly
The Female Athlete Triad
I want to specifically address a pattern I see too often in young female athletes that goes unrecognized for months: the Female Athlete Triad.
It is the dangerous combination of:
- Low energy availability (often from disordered eating)
- Menstrual dysfunction (missed or irregular periods)
- Low bone density
Female athletes with this triad are at very high risk of recurring stress fractures and long-term bone health problems. If a young woman presents with a second or third stress fracture, this triad must be screened for — it is a medical issue, not just a training error.
Who Is Most at Risk?
High-Risk Groups
- Endurance runners — especially those who overtrain or rapidly increase mileage
- Military recruits — the rapid transition to high-volume marching is a textbook cause of metatarsal stress fractures
- Ballet dancers and gymnasts — high impact, low body weight, often suboptimal nutrition
- Basketball and tennis players — repetitive jumping and lateral movements
- Postmenopausal women — declining estrogen accelerates bone density loss
- Men over 50 — testosterone decline can also reduce bone density over time
Risk Factor Checklist
| Risk Factor | Why It Increases Risk |
|---|---|
| Recent significant increase in activity | Bone remodeling can’t keep up |
| Low BMI or history of eating disorder | Insufficient nutritional support for bone health |
| Vitamin D level below 30 ng/mL | Impairs calcium absorption and bone mineralization |
| Prior stress fracture | Indicates underlying vulnerability |
| Flat feet or high arches | Alters load distribution across foot bones |
| Irregular or absent menstrual periods | Signals low estrogen, which is protective for bone |
| Smoking | Impairs bone healing and remodeling |
How Is a Hairline Fracture Diagnosed?
Clinical Examination
Before any imaging, a good orthopedic examination tells you a great deal. I assess:
- The exact location of point tenderness
- Whether a “hop test” (single-leg hopping on the affected limb) reproduces the pain
- The “fulcrum test” for tibial fractures — applying bending force to the leg
- Range of motion and gait analysis
Imaging Options
| Test | Sensitivity for Hairline Fracture | When I Use It |
|---|---|---|
| X-ray | Low (10–20% in first week) | First step — rules out complete fracture; fracture line may appear after 2–3 weeks as bone heals |
| MRI | Very high (>90%) | Gold standard — shows bone marrow edema before a visible crack; best for foot, ankle, hip |
| Bone scan | High but non-specific | Detects increased bone metabolism; can’t differentiate fracture from infection or tumor; rarely used now that MRI is accessible |
| CT scan | High for specific sites | Best for navicular, vertebral, and femoral neck fractures; provides 3D detail |
A critical point for patients: If your doctor orders an X-ray that comes back “normal” but you still have significant point tenderness and activity-related pain, push for an MRI. I have seen patients told they are fine after a normal X-ray, who had a stress fracture that was only visible on MRI. The X-ray misses early hairline fractures far more often than it catches them.
Treatment of a Hairline Fracture
Conservative Treatment (First Line for Most Fractures)
The vast majority of hairline fractures — perhaps 85 to 90 percent in my practice — heal completely with non-surgical management. The cornerstone is simple but non-negotiable: remove the load.
The RICE Protocol (Immediate Management)
- Rest — stop the aggravating activity entirely; this is not “reduce the activity,” it is stop
- Ice — 15–20 minutes every 2–3 hours in the first 48 hours to manage swelling
- Compression — light elastic bandage around the area
- Elevation — keep the limb elevated above heart level when resting
Medical Management
- Protected weight-bearing: Crutches for lower limb fractures to remove load from the bone
- Walking boot or cast: A rigid boot or short-leg cast immobilizes the foot and reduces stress on healing bone — very commonly prescribed for metatarsal and tibial fractures
- NSAIDs: Ibuprofen or naproxen for pain and inflammation in the short term; however, there is some evidence that long-term NSAID use may interfere with bone healing, so I typically limit use to the first week
- Vitamin D and calcium supplementation: If blood levels are low (Vitamin D below 30 ng/mL or calcium intake inadequate), supplementation is started immediately
Typical Timeline for Return to Activity
| Fracture Site | Healing Time | Return to Sport |
|---|---|---|
| Metatarsal (2nd/3rd) | 6–8 weeks | 8–12 weeks |
| Tibia | 6–10 weeks | 10–14 weeks |
| Fibula | 4–6 weeks | 6–10 weeks |
| Calcaneus | 6–8 weeks | 8–12 weeks |
| Navicular | 8–12 weeks | 12–16 weeks |
| Femoral neck | 8–12 weeks (with surgical assessment) | 12–20 weeks |
The single biggest mistake patients make: They feel better after 3 weeks and resume full activity. Pain disappearing does not mean the fracture has healed. Bone remodeling and complete structural repair take 6–8 weeks minimum. Resuming too early is how a hairline fracture becomes a complete fracture requiring surgery.
Surgical Treatment
Surgery is considered in the following situations:
- High-risk fracture sites that have poor blood supply and high non-union rates (navicular, femoral neck, anterior cortex of tibia)
- Fractures that have not healed despite adequate conservative management (non-union after 3–4 months)
- Complete displacement of the fracture fragments
- Athletes with time-sensitive return requirements — in elite sport, surgery with internal fixation sometimes allows faster controlled rehabilitation
Surgical options typically include percutaneous screw fixation for small bones (navicular, metatarsal) or intramedullary nailing for tibial fractures.
Complications of Untreated or Undertreated Hairline Fractures
This is the section I wish every patient read before deciding to “walk it off.”
- Complete fracture — the crack propagates through the entire bone, requiring casting or surgery and significantly longer healing time
- Non-union — the fracture fails to heal, resulting in persistent pain and possible chronic instability; more common at high-risk sites with poor blood supply
- Avascular necrosis — blood supply to the bone is disrupted, causing bone death; can occur with femoral neck and navicular fractures
- Chronic stress reaction — recurring pain at the site even after apparent healing; often indicates the underlying cause (training error, nutritional deficiency, bone density issue) was never addressed
- Recurrence — without identifying and correcting risk factors, stress fractures have a high recurrence rate
Recovery: What to Do While You Heal
Healing from a hairline fracture does not mean doing nothing. It means doing the right things.
What You Can Do
- Swimming — full cardiovascular and upper body workout with zero lower limb impact
- Pool running — wearing a flotation vest and running in deep water maintains running-specific fitness without any bone loading
- Cycling (stationary or road) — low-impact, excellent for maintaining leg strength and cardiovascular fitness
- Upper body strength training — maintain general fitness and muscle mass
- Core strengthening — valuable for all athletes; can be performed without weight-bearing through the fracture site
What to Avoid
- Running, jumping, or any high-impact lower limb activity
- Going barefoot on hard surfaces if you have a foot or ankle fracture
- Resuming activity just because pain has resolved
Nutrition During Recovery
Bone healing is an active metabolic process that requires fuel.
- Calcium: 1,000–1,200 mg/day (dairy, leafy greens, fortified foods, or supplement)
- Vitamin D: 1,500–2,000 IU/day if deficient; maintain blood levels above 30 ng/mL
- Protein: Adequate protein intake supports bone matrix repair
- Collagen-supporting nutrients: Vitamin C is necessary for collagen synthesis, which forms the organic matrix of bone
Preventing Hairline Fractures
Prevention is significantly more straightforward than treatment. In clinical practice, I advise patients — particularly athletes — as follows:
Training Principles
- Follow the 10% rule: never increase weekly mileage or training volume by more than 10% from the previous week
- Build in rest days — bone remodeling requires recovery time; rest is not weakness, it is adaptation
- Alternate high-impact with low-impact training days
- If switching sports or surfaces, allow a gradual adaptation period of 4–6 weeks
Equipment
- Replace running shoes every 400–600 miles (approximately 640–960 km)
- Use shoes appropriate to your foot type (gait analysis at a specialist running store is worthwhile)
- Consider custom orthotics if you have significant flat feet or high arches
Bone Health
- Get a Vitamin D blood test annually if you are an active adult, especially in low-sunlight regions
- Ensure adequate dietary calcium
- Women approaching or past menopause should discuss bone density screening (DEXA scan) with their doctor
Warning Signs to Act On Immediately
- Pain that persists past the end of a training session
- Pain that wakes you at night
- Any point tenderness directly on bone (not muscle or ligament)
- Swelling over a bone after exercise
Frequently Asked Questions
Can I walk on a hairline fracture? Technically yes in some cases, but clinically I advise against it. Walking continues to load the fracture, slowing healing and increasing the risk of complete fracture. If your doctor has prescribed a walking boot, wear it consistently — not just when it hurts.
How do I know if I have a hairline fracture or a sprain? The classic differentiator is point tenderness directly on bone (fracture) versus around a ligament (sprain), combined with the gradual onset of pain that worsens with activity. An MRI gives a definitive answer when clinical examination is uncertain.
Will a hairline fracture show on an X-ray? Often not in the first 1–2 weeks. The fracture line may become visible later as the bone begins to heal and the healing callus calcifies. MRI is far more sensitive for early diagnosis.
Can a hairline fracture heal on its own without seeing a doctor? Some low-risk fractures (e.g., minor metatarsal fractures) can heal with rest alone, but there is no way to know whether you have a low-risk or high-risk fracture without imaging. Femoral neck and navicular fractures missed at home can have serious permanent consequences. Always get evaluated.
How long does a hairline fracture take to heal? Most fractures are substantially healed at 6–8 weeks, but full bone remodeling and return to unrestricted sport can take 10–16 weeks depending on the site. Nutritional status, age, and adherence to rest all influence healing time.
Can stress fractures come back? Yes, and they frequently do when the underlying cause — training error, nutritional deficiency, or bone density issue — is not addressed. A recurrence should prompt a thorough workup including Vitamin D, calcium, hormonal status, and bone density testing.
When to See an Orthopedic Specialist
See a doctor promptly if:
- You have point tenderness directly over a bone that does not improve with a few days of rest
- You have pain after a significant increase in activity
- Your X-ray is normal but pain persists
- You have had a previous stress fracture
- You are an older adult (over 50) with new bone pain after activity
- You are a female athlete with irregular periods and recurring bone injuries
You should go to the emergency room if:
- You cannot bear any weight at all
- You heard a snap or pop and have significant swelling and bruising
- There is visible deformity
- You suspect a hip or femoral neck injury
Conclusion
A hairline fracture is the body’s signal that it has been asked to do more than it can currently handle. The good news is that with proper diagnosis, appropriate rest, and attention to the underlying risk factors, the overwhelming majority of patients heal completely and return to full activity.
The mistakes that turn a 6-week recovery into a 6-month ordeal are almost always the same: delayed diagnosis, continued loading through the pain, and premature return to activity. Respect the fracture, address the cause, and give the bone the time and nutrition it needs to repair.
If you are experiencing symptoms described in this article, find a verified orthopedic specialist on Doctiplus to get an accurate diagnosis and a personalized recovery plan.
Disclaimer
This article is written for informational purposes and does not constitute individualized medical advice. Always consult a qualified orthopedic physician for diagnosis and treatment.
References
- May T, et al. (2023). Stress fractures. StatPearls [Internet]. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK554538/
- American Academy of Orthopaedic Surgeons. Stress Fractures. OrthoInfo. https://orthoinfo.aaos.org/en/diseases–conditions/stress-fractures/
- Warden SJ, et al. (2014). Stress fractures: pathophysiology, epidemiology, and risk factors. Current Osteoporosis Reports, 12(3), 291–303.
- Kahanov L, et al. (2015). Diagnosis, treatment, and rehabilitation of stress fractures in the lower extremity in runners. Open Access Journal of Sports Medicine, 6, 87–95.
- Nattiv A, et al. (2007). American College of Sports Medicine position stand: The female athlete triad. Medicine & Science in Sports & Exercise, 39(10), 1867–1882.
Dr. Noah Finkel, MD is a distinguished orthopedic surgeon practicing in Huntington, New York. He earned his Doctor of Medicine from the State University of New York, Upstate Medical University, completed his internship at Bellevue Hospital Center, and advanced his training with a fellowship at New York University and Mount Sinai Hospital.